http://cepr.net/publications/op-eds-columns/reducing-the-health-care-tax
Jared Bernstein and Dean Baker
The Washington Post, January 14, 2020
One of most enduring, economically and socially damaging, downright frustrating facts about life in the United States is how expensive health care is here. Not only does U.S. health care cost far more than in other advanced economies, but compared with the nations that spend less, we have worse or equivalent health outcomes. In fact, U.S. life expectancy now lags behind that of all the advanced economies.
An MRI scan that cost $1,400 here went for $450 in Britain and $190 in Holland. Thirty tablets of a drug to reduce the risk of blood clots (Xarelto) cost $380 here, $70 in Britain, $80 in Switzerland and $60 in Holland. Hospital admission for angioplasty is $32,000 here, $15,000 in Australia, $12,000 in Britain, $7,000 in Switzerland, $6,000 in the Netherlands.
Add to those differences the latest outrage in health-care costs: surprise medical billing, when even well-insured patients can wake up from surgery finding that they owe thousands of dollars, because someone treating them while they were unconscious was out of their insurance network.
Princeton economists Anne Case and Angus Deaton (a Nobel winner) recently summarized the problem by labeling it an $8,000-a-year annual health-care tax paid by U.S. families. This is the difference in costs between what we pay for health care and what people in other countries pay. As Case put it: "We can brag we have the most expensive health care. We can also now brag that it delivers the worst health of any rich country."
Why call this expense a tax? Well, for one, if you want health coverage, you can't escape it. But even if you don't — and good luck with that — you still can't escape the tax, as both employer- and government-provided health care extract payments through lower paychecks and public financing.
Case and Deaton may be erring on the low side in their $8,000-per-family figure. The Organization for Economic Cooperation and Development puts per-person spending in the United States at $8,950 a year. That compares with $5,060 in Germany, $3,470 in Canada and just $3,140 in Britain. If we assume a family of three, we would get an annual health-care tax of $11,670 compared with Germany and more than $17,000 compared with the cost of health care in Britain.
How can such differences persist, especially in a service where consumption is so essential to well-being? If ice cream were that much more expensive here, we'd have a lot to squawk about, for sure. But it wouldn't be a matter of life and death.
An obvious, and correct, answer as to why U.S. health care is so expensive is because we do so little, relative to other systems, to control costs. But it's worse than that. We do a fair amount to make health care more expensive.
First, our system of private insurance costs far more than single-payer systems like Canada's, and also more than countries with private but heavily regulated insurers like Germany. OECD data show that as a share of health spending, our administrative costs are three times that of Canada's and twice that of Germany's. Getting our administrative costs closer to those in other countries would require regulating private insurers and expanding public coverage, but it could save us at least 10 percent of our total health-care bill.
Next, we pay twice as much to our health-care providers and for prescription drugs as everyone else. The latter costs us more than $3,000 per family per year. We pay more than twice as much for medical equipment, costing us a bit less than $1,500 per family per year. Doctors and dentists cost us close to an extra $750 per family per year.
One reason for the outsize costs of these inputs to U.S. health care is that government policy protects our providers. When it comes to manufactured goods, like cars and clothes and almost everything on the shelves of Walmart, economists and policymakers push for "free trade" and more competition. But when it comes to health-care providers, these same authorities turn protectionist.
In areas like prescription drugs and medical equipment, this protection is explicit: Manufacturers are granted patent monopolies. The government will arrest anyone who sells protected items in competition with a patent holder.
In the case of doctors, we have maintained or increased barriers that make it difficult for qualified foreign physicians to practice in the United States. We also prevent other health-care professionals, such as physicians' assistants and nurse practitioners, from doing many tasks for which they are entirely competent. There is a similar story with dentists and dental hygienists.
Other countries directly control drug prices. In France, the government determines whether a new drug is an improvement or a copycat, and, if the drug is deemed useful, the government negotiates drug prices with the manufacturers and caps their revenue. When sales exceed the cap, the manufacturer must rebate most of the difference back to the government.
Here in the United States, we give drug companies and medical equipment manufacturers' patent monopolies and allow them to charge whatever they want. We don't even let the government use its massive leverage to negotiate lower drug prices for Medicare beneficiaries. That's what makes these goods expensive; they're almost always relatively cheap to produce.
This is fixable. It would take regulating costs, reducing reimbursements to providers and increasing competition.
The pharmaceutical industry's rationale for cost-exploding medical patents is that it helps incentivize research and innovation. Without them, it's likely that pharmaceuticals and medical equipment companies would do less speculative research. But it would take a fraction of the savings from reducing such protectionism to replace patent-support research with publicly supported research (for which we already spend $40 billion a year).
In terms of boosting competition, allowing foreign doctors whose training meets our standards to more easily practice medicine here would bring U.S. physicians' pay in line with international standards. Of course, our doctors pay much more for their education than doctors trained elsewhere, so part of this new structure would also require reducing the domestic cost of medical education and alleviating some of the educational debt burden that U.S.-trained doctors have acquired.
Increasing competition would also require using antitrust measures to push back on the pricing power engendered by the consolidation of both hospital groups and medical practices. An analysis by the New York Times of 25 metro areas found that hospital mergers "have essentially banished competition and raised prices for hospital admissions."
Even if we succeed in raising competition and reducing protectionism, health care will still be too expensive for many low- and moderate-income families, many of whom have suffered stagnant incomes in recent decades. Like every other wealthy country, we will need to get on a path to universal coverage. But whatever form that takes, if we can significantly reduce our current health-care tax, the savings will easily be large enough to extend quality, affordable coverage to every American.
-- via my feedly newsfeed







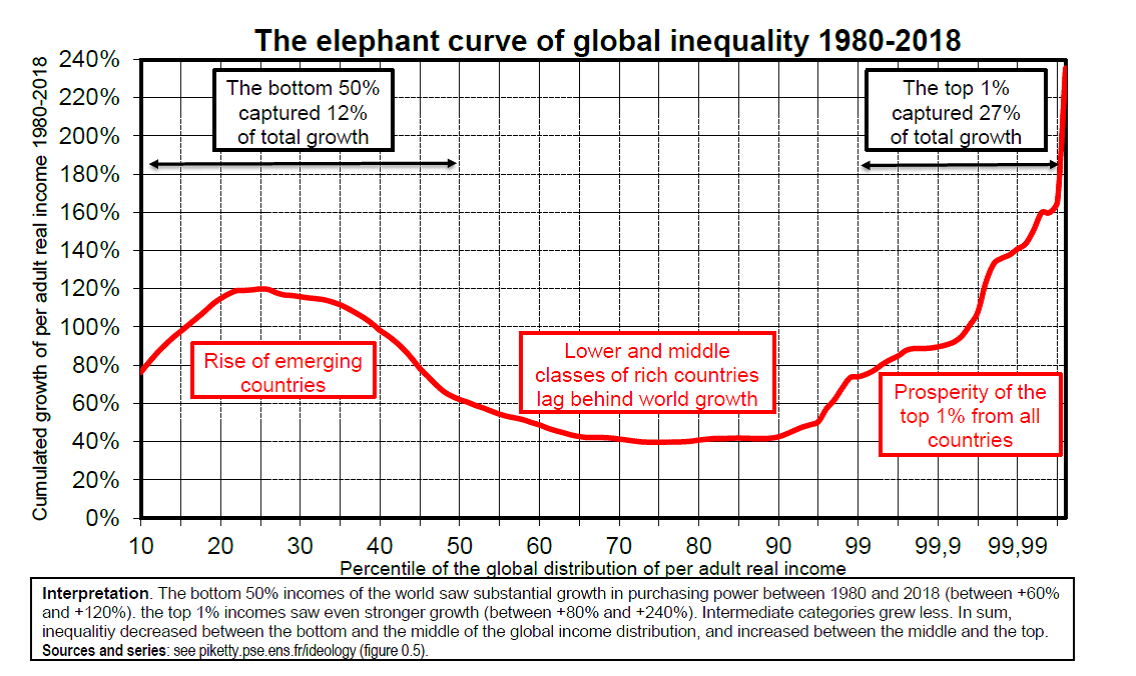 In the wake of the denial of global warming, now on the wane, at least superficially, are we at present witnessing the denial of the rise in inequality?
In the wake of the denial of global warming, now on the wane, at least superficially, are we at present witnessing the denial of the rise in inequality?