http://cepr.net/publications/op-eds-columns/can-we-pay-for-single-payer
Dean Baker
Democracy, September 14, 2017
Building off momentum from his campaign and the defeat of the Republican efforts to repeal and replace Obamacare, Bernie Sanders has come out with a new proposal, backed by 16 other senators, to phase in a single-payer health-care plan. This plan is more modest in several ways than the one put forward in his campaign—most notably, it does not look to get to a universal Medicare-type system in a single step. In this way, the new proposal offers enormous opportunities for slicing and dicing that can get us to single payer incrementally. This is good news because getting there all at once, as Sanders proposed in his campaign, was almost certainly not a doable task.
There are many reasons why a move to single payer is attractive. Single-payer systems have been successful in providing universal care to the populations of the countries that have them, and doing so at a far lower cost than in the United States. Per-person health-care costs in Canada are 47 percent of the costs in the United States. The per-person cost for the single-payer system in the United Kingdom, where health care is provided directly by the government, is 42 percent of the U.S. system. These and other single-payer countries do better than the United States on broad outcome measures like life expectancy and infant mortality and are comparable on more narrow measures like survival rates from various types of cancer and other diseases.
The logic of single payer is simple. If we want to ensure that everyone gets a decent level of health care, it doesn't make sense to have competing insurers. There are economies of scale from having a single system. Competing insurers will add a layer of unnecessary costs. Furthermore, since insurers make money when they don't provide care, the government will have to devote resources to regulating insurers to be certain they provide necessary treatment options to patients.
The economies of a single system can be viewed as analogous to the Social Security system, which has administrative costs that are less than 1/20thas much as privatized systems in places like Chile and the United Kingdom. The analogous institution in the health-care sector is of course Medicare, which has administrative costs of less than 2 percent of benefits in the traditional fee-for-service portion of the program, roughly a tenth the cost for private insurers. Markets are great in situations where we expect individuals to exercise choice, but when we want to ensure a basic standard—a minimal retirement income in the case of Social Security or good quality health care in the case of Medicare—there is a lot to be said for the efficiency of the one-size-fits-all approach.
While a single-payer system is probably the most efficient way to provide universal coverage, it is not the only way. Most wealthy countries do not provide coverage to their population through single-payer systems. Many countries, including Germany, France, and the Netherlands, provide coverage through heavily regulated non-profit insurers. This is important to keep in mind, since it means we can have universal health-care coverage without single payer.
It's not clear that it is a good thing for progressives to gain power if they are committed to a program that really is unworkable policy.
Nonetheless, a single-payer system would undoubtedly offer savings in administrative costs. There also is an advantage stemming from the fact that it has been the focus of a major progressive health-care reform movement, led by the Physicians for a National Health Program and National Nurses United, for more than a quarter century. And single payer, or Medicare for All, does have a seeming simplicity to it, which is a huge advantage for any political effort.
Yet in spite of the economic and political benefits of a single-payer system, there almost certainly is no direct path that gets us to such a system from where we are today. The basic problem is that the move to single payer involves a massive shift of resources. It would imply taking an amount equal to almost 10 percent of GDP ($1.9 trillion in the economy of 2017) that is currently spent by the private sector and instead having it spent by the federal government. Furthermore, it would require the restructuring of the 7 percent of GDP that the government already spends on health care through Medicare, Medicaid, and other government health programs.
This is a massive rechanneling of resources, which is difficult to envision going smoothly. Among other things, we could not guarantee that people would be able to keep their doctors, since many may consider the compensation rate too low and opt out of the system or take relatively few patients who are in the system. While many single-payer advocates would like to prohibit doctors from practicing outside the system, it would be a huge political lift to prohibit such practices. Furthermore, the current Supreme Court would almost certainly strike down a ban on outside practices as unconstitutional. It is worth noting that even countries with universal single-payer type systems, like the United Kingdom and Denmark, have private systems that operate in parallel with the public one, although in the UK, for example, doctors must practice at least 40 hours a week in the NHS, avoiding a completely bifurcated system.
The proponents of single payer often point to the creation of Medicare as a model. But in 1966, the first year of Medicare's existence, the program spent an amount that was less than 0.3 percent of GDP at the time. Even by 1970, year five of the program's existence, spending was just over 0.7 percent of GDP. When other countries adopted single-payer systems they were generally spending less than one-fifth as much of their economy on health care as the United States does today. Even then, they did not necessarily go this route in a single step. In Canada, which is often viewed as a model for the United States, the system was pioneered by a single province before being implemented nationally. Needless to say, people who saw the government struggle with setting up a website for Obamacare might be skeptical of its ability to take control of $1.9 trillion in annual spending in a short period of time.
However the most immediate issue in a transition to single payer is finding a way to finance such a large amount of spending through the government. Basically, we need a way to tax people, by an amount roughly equal to what they now pay in premiums and out-of-pocket expenses. Having worked with the single-payer advocates in Congress on this issue in years past, I can say that it is not easy. While in principle it should be a matter of indifference to people whether they pay money for health insurance to providers in the form of premiums and co-payments or to the government in the form of taxes, members of Congress who have to run for reelection don't seem to think this is the case. For my part, I was not able to construct a revenue package that single-payer advocates would agree to. Instead we adopted a menu of options. Of course, for an actual bill, Congress needs specific revenue sources, not a menu.
University of Massachusetts economist Gerald Friedman bravely picked up this job for the Sanders campaign, as he tried to design a plan to pay for the single-payer proposal Sanders put forward in his campaign. I think it's fair to say the plan comes up somewhat short. Even with generous assumptions about potential revenue and savings, there would still be a substantial gap between the additional spending and the new revenue.
There are two tasks involved in calculating the revenue needed to fund single payer. The first is to determine the total amount of revenue that would be needed. The necessary revenue depends in turn on assumptions about the increased use of medical services as a result of universal coverage and also the elimination of most deductibles and copays patients face under the current system, even if they have private insurance or Medicare. The assumption for needed revenue also depends on the savings that could be expected from introducing a single-payer system. This includes both savings on administrative costs and also reduced payments for prescription drugs and other items. The additional expenses minus the assumed savings provide the basis for the revenue target.
That brings up the second part of the story: putting together a mix of taxes that would be enough to cover the additional expenses incurred by the federal government. It is worth noting in this respect that the revenue must go to the federal government since the assumption is that expenses currently borne by state governments, such as payments for Medicaid and the State Children's Health Insurance Program, will instead be paid by the federal government.
Calculating the Revenue Target
According to Friedman's calculations, we get the mix of additional expenses and savings shown in Table 1.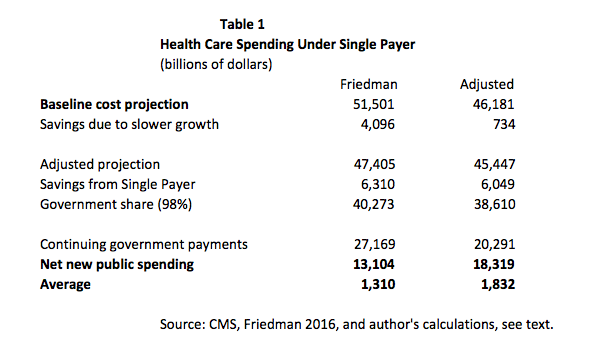
This leaves a projected gap of $13.8 trillion over the 10-year budget horizon from 2017 to 2026, which averages $1.38 trillion annually. I have substituted my alternative calculations in the right column. (The starting point in my assessment is the most recent projection from the Centers for Medicare and Medicaid Services (CMS), which differs somewhat from the older one used by Friedman.)
The first big difference is the assumption on the difference in cost growth. Friedman assumes that adopting a single-payer system would slow the growth of annual health-care costs by 1.1 percentage points relative to the baseline due to the gap in growth in costs between the United States and Canada and also the gap in per-person cost growth in private insurance and Medicare. In recent years, the growth of health-care costs has slowed sharply. CMS projects that per-person cost growth for private insurance will exceed the growth rate for Medicare by 0.46 percentage points annually. My calculation applies this difference in spending to the CMS projection for private sector insurance costs. This gives savings of $734 billion rather than the $4,096 billion in Friedman's calculation.
The next item is the assumed savings from a single-payer system, combined with the increased cost associated with more utilization as a result of making most health care available at no cost. The projected savings would result from both eliminating the excess administrative costs associated with the private insurance system and also from negotiating drug prices with the pharmaceutical industry. I have accepted the same ratio, 13.4 percent, of total savings as Friedman, although it is arguably over-optimistic.
The figure first of all assumes that the pure overhead costs for administering the program would be 2 percent, a bit more than the costs of Medicare. This can be viewed as optimistic since at least some of the costs for insurance are going to be proportional to the number of people enrolled. Medicare patients on average have slightly more than twice the per-person health-care costs as the people covered by private insurance. If the per-person costs for covering people on a single-payer system were the same as for Medicare then they would be close to 4 percent of payouts, rather than the 2 percent assumed by Friedman.
The numbers also assume large savings for providers based on the assumption that they will need fewer workers to deal with the paperwork that is necessary for dealing with multiple insurers. These calculations are based on research comparing administrative overhead for U.S. providers with providers in Canada. While the projected savings are certainly plausible, it is worth noting how they would be realized. The savings would come from providers, such as hospitals, doctors' offices, and nursing homes, cutting back on their staff. People leave their jobs all the time and it's not uncommon for hospitals and other employers in the health-care sector to lay off workers, but it seems unlikely the adjustment to a new system with fewer administrative staff will be achieved overnight. In other words, these savings may be what are seen after an adjustment period of several years, but not immediately.
The last major category of savings is on payments for prescription drugs. Friedman assumes savings on prescription drugs of 37.5 percent. This might actually be too low. Friedman's figure assumes that we pay the same amount for our drugs as the average for other wealthy countries. This is a reasonable starting point, but it is important to realize that drugs are almost always cheap to produce. They are expensive to buy because we give drug companies patent monopolies and other types of protection that allow them to charge prices that can be many thousand percent above the free market price.
The case of the Hepatitis C drug Sovaldi provides a dramatic example. The retail price in the United States was set by Gilead at $84,000. A high quality generic version is available in India at $300 per treatment. Patent monopolies are intended to provide incentive to conduct research; however there are other ways to provide this incentive. For example, we could directly contract with firms to do the research, as the Army recently did with Sanofi to develop a Zika vaccine. (Unfortunately, the Army agreed to give Sanofi a monopoly on the vaccine, even though the Army is paying for the research and clinical tests.)
The potential savings from financing research upfront and then having drugs sold in a free market are enormous. We are on a path to spend more than $450 billion in 2017 on prescription drugs. And, in a free market, these drugs would likely sell for less than $80 billion. Even if we added in $60 billion in public funds to replace research currently supported by patent monopolies, it would still imply savings of almost 70 percent.
There is a similar story with medical equipment. We will spend almost $90 billion in 2017 on the purchase of medical equipment. Even the most complex scanning machine is relatively cheap to manufacture. Here also it is the patent monopolies that make them expensive. Paying for the research upfront can lead to savings on medical equipment of the same magnitude as the savings on drugs noted above. If changes in the financing of medical research accompanied a shift to single payer, Friedman's calculations of aggregate savings would certainly be reasonable.
The assumptions on increased utilization may be overly optimistic. Friedman assumes substantial increases in utilization for the currently uninsured, as well as large increases for newly covered services like home health care and nursing home care. However, he assumes relatively little increase in services for those who are already insured but face substantial co-pays and deductibles with their current plans. There is evidence that these out-of-pocket expenditures have a substantial impact on reducing spending, most notably the gap between per-person spending by people with relatively generous insurance plans and people with plans that have large deductibles and high co-pays. However, if we accept Friedman's assumptions on the changes in utilization, the net increase in spending comes to 5.3 percent. This includes the government's assumption of Medicare Part B premiums and also an increase in the provider compensation rates for Medicaid to Medicare levels.
The next line is the assumption that 98 percent of health-care costs would be covered by the government. The remaining 2 percent would be money that people would expected to pay for things like cosmetic surgery, non-prescription drugs, and other relatively low-cost and/or optional spending. It's worth noting that this is an extremely optimistic expectation for out-of-pocket spending. It implies that we would spend roughly 0.3 percent of GDP on OOP. That compares to 1.9 percent at present. However, the 0.3 percent figure would put us well below all other countries, including France at 0.7 percent, and Canada and the United Kingdom, two single-payer countries, both at 1.4 percent. In my calculation, I have applied the same 0.98 percent ratio. This gives the total spending that must come from the federal government over the next decade: $40.273 trillion in Freidman's calculations and $38.61 trillion in my calculations.
Then, the amount the government is currently projected to spend over the next decade is deducted. Friedman uses the baseline projections from CMS. This is likely too high since it assumes that state and local governments will continue to pay at the same rate as the baseline. While the federal government does often have maintenance of effort rules for state and local governments (meaning they continue to spend the same amount of money even though a program has been qualitatively changed), this one might be too big of a reach given the Supreme Court ruling that overturned the ACA requirement that states expand Medicaid. In this case, the baseline assumes substantial increases in real spending over the next decade and also that state and local governments would continue to make premium payments for employees who are being covered by Medicare for All.
My calculation assumes that state and local governments will make 80 percent of the projected payments for Medicaid and other programs, as well as continuing all payments that would have otherwise gone for insurance premiums for their workers. (It is worth noting that reductions in spending from the baseline should mean lower taxes at the state and local level, other things being equal.) That is likely substantially more than could reasonably be expected. My net new costs for the government come to $18.319 trillion compared to Friedman's $13.104 trillion, a difference of more than $5 trillion, or more than $500 billion a year.
I also see some differences in my calculations on the revenue side of the equation. I have reproduced Friedman's calculations alongside my own in Table 2. Since most of the projections are reasonable, I will only mention the two where I have notable differences.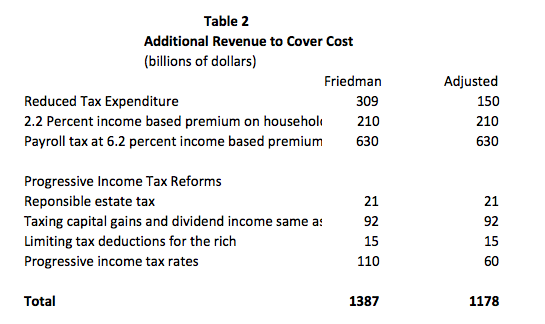
The first is the calculation for the savings on tax expenditures. Most of the tax expenditures on health care are from employer paid insurance, which is not subject to either income or payroll tax. The expectation is that if we ended employer-provided insurance, wages would rise by roughly an amount equal to what employers are now paying for insurance. This would not happen immediately and not for all workers, but as an average this is probably a good working assumption.
However, wages would not rise by the full amount of the premium if we are requiring employers to pay a 6.2 percent tax on wages to cover the cost of single payer. This would imply that wages are roughly $630 billion less than they would be if employers didn't pay the tax or the premium. This is money that would escape both the income tax and the payroll taxes for Social Security and Medicare. (Also, since state and local governments are still expected to be paying an amount equal to current premiums for their employees, the pay for these workers would be lower rather than higher.) This leaves an adjusted savings on tax expenditures of $150 billion. (I calculated the difference by assuming a 15.35 percent payroll tax on the $630 billion, plus a 20 percent average marginal income tax rate. I did not factor in the roughly $260 billion in annual premium payments that state and local governments would be expected to continue making, which presumably means that wages for these workers would be correspondingly lower.)
The other change is in the calculation of the revenue from higher income taxes. I have assumed that the yield from the higher taxes in the Sanders proposal from his campaign would be $60 billion a year, as opposed to the $110 billion assumed by Friedman. This is based on the Congressional Budget Office's projection that raising the tax rate on everyone in the 28 percent bracket or higher by 1 percentage point would raise $15 billion a year. The structure laid out in the campaign proposal is more complicated with the highest earners (above $10 million a year) seeing a 12.4 percentage point increase in their marginal tax rate, but I have assumed that the total package will be roughly equal to a 4 percentage-point increase in the tax rate for those in the 28 percent bracket and above.
The revenue from raising taxes will not be proportionate to the percentage point change in the tax rate, since people will have more incentive to conceal their income or to simply earn less when their rate gets very high. For the high earners facing an increased tax rate, this would be in addition to the 2.2 percentage point premium that is imposed on middle-income earners and above. For those in the highest income bracket, the effective federal tax rate would then be 58 percent (a 52 percent income tax rate, the 2.2 percent Medicare for All premium, and the 3.8 percent tax for Medicare/Obamacare). If we add state income taxes, which are as high as 13.3 percent in California, it is reasonable to believe that there will be serious efforts at avoidance as well a real disincentive effect. This is not an issue of how we feel about the very rich and whether they are over-taxed, it is a question of how they respond to higher tax rates. And existing research suggests that the revenue gains from pushing tax rates to these levels are very limited. For this reason, the $60 billion figure assumed in my calculation is likely an optimistic number.
The sum for increased revenues in my calculation is $1.178 trillion: This comes to a bit more than $200 billion under the figure calculated by Friedman. Coupled with the differences on the spending side, this leaves gap of more than $650 billion a year or $6.5 trillion over a ten-year budget horizon. This is real money, even in the context of the federal budget. To give a comparison, this is roughly ten times as much money as was at stake with the Republican proposals to repeal Obamacare. On a per-person level, the funding gap would be a bit under $2,000 per person per year.
If the idea is to get to single payer in a single step, it would take lot more money to get there than the Sanders plan is proposing to raise. There are always more steps that can be taken to try to reduce costs further or raise other taxes, but these are not likely to be popular. These steps involve making the plan less generous, doing more to reduce the income of providers, raising taxes on people who are not rich, or some combination.
These are all general suggestions; legislators would have to decide how far they want to go on each.
Single Payer with a Shortfall
In short, a single-payer plan that has more realistic projections is not likely to look very good to many people who would be happy to put the insurance industry out of business. It's possible that pushing for the plan Sanders has outlined, without being more specific about the costs, could be an effective political strategy. After all, plenty of Republicans have been elected with promises that clearly do not add up.
But my guess is that this will not prove a winning strategy for progressives. The right can count on rich and powerful allies to push their case even when they are not telling the truth. This power is generally sufficient to get them to the he said/she said space in major news outlets, where respectable people are supposed to treat their arguments as being serious, even if they are ludicrous on their face.
Progressives do not have this luxury. In fact, we got a taste of how the mainstream and even somewhat liberal media might respond to a single-payer plan that does not add up during the Sanders campaign. Health economist Kenneth Thorpe did an analysis of Sanders's plan and found an annual shortfall of $1.4 trillion. This was quickly seized upon in reporting and opinion pieces in places like The Washington Post and Vox. The latter even put up a tax calculator in which much of the projected shortfall in Sanders's health-care plan was filled with a regressive payroll tax. This allowed them to push the line that Sanders had a "soak the poor" tax agenda.
There is also a question of what the policy would be if progressives actually took power. What would a Democrat who ran on a single-payer plan like the one pushed by Sanders do if she actually was in the White House? Would she be able to back down and offer less than promised? Perhaps, but this is something worth considering. It's not clear that it is a good thing for progressives to gain power if they are committed to a program that really is unworkable policy. That has generally not proven to be a good long-term strategy for advancing progressive goals.
There are many steps that can be taken to rein in costs and extend coverage that are short of a big leap to single payer. Lowering the age of Medicare eligibility to 55, as the new Sanders plan proposes, would be good a start, along with allowing a buy in for people at younger ages. We can also look for some of the cost savings envisioned under single payer, most notably public funding of research for prescription drugs and medical equipment so these items can be sold in a free market without patent protection. And, we could be looking to get the pay of our doctors and dentists down to the levels in other wealthy countries, which would save us close to $100 billion a year from our health-care bill.
The target of eliminating almost all out-of-pocket expenses may also be too ambitious. If we set the target at 1.4 percent of GDP, the same as people in Canada and the UK now pay, instead of the 0.3 percent in the Sanders's plan, it reduces the annual shortfall by $250 billion, apart from any impact on utilization. And it wouldn't really mean much hardship for most of the population. For example, if a family earning $100,000 a year was expected to spend $1,600 annually on various health-care expenses, it is hard to see this imposing a great burden.
In short, the current political environment is presenting a great opening for progressive health-care reform. This opening could be wasted if progressives are not willing to work for a wide range of reforms that would extend coverage and reduce costs and, instead, insist on a single-minded focus on single payer. The new proposal that Sanders put forward with 16 Senate co-sponsors offers the sort of flexibility needed to structure a workable incremental approach. This is a huge step in the right direction.
-- via my feedly newsfeed

No comments:
Post a Comment